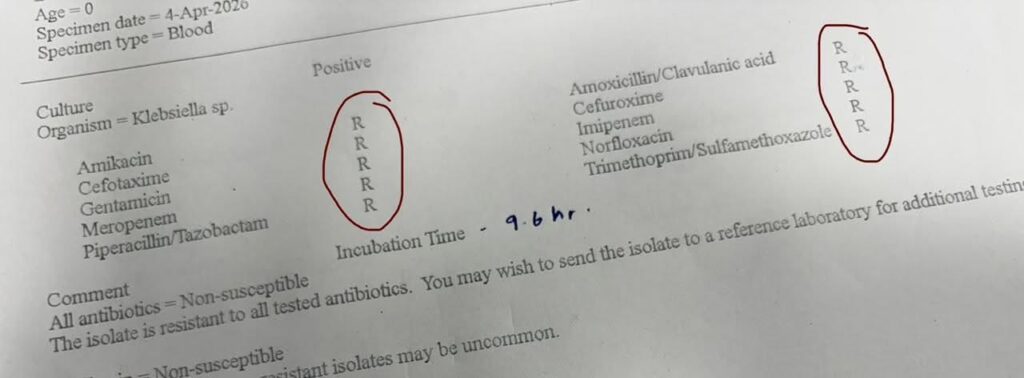
A laboratory report dated 4 April 2026 has sent shockwaves through Sri Lanka’s medical community. A blood culture from a newborn infant grew Klebsiella species that proved resistant to every single antibiotic tested (Pan-Resistant Bacteria) including last-resort drugs such as meropenem, imipenem, amikacin, piperacillin-tazobactam, and cefotaxime. The comment on the report is blunt: “All antibiotics = Non-susceptible. The isolate is resistant to all tested antibiotics.” The laboratory recommends sending the sample to a reference lab for further testing, but the immediate reality is stark standard treatment options are exhausted.
This is not an isolated laboratory curiosity. It is a clear warning of the growing crisis of antimicrobial resistance (AMR) in Sri Lanka, where multi-drug resistant and extensively drug-resistant bacteria are becoming more common in hospitals and communities.
Also in Explained | The Antibiotic Crisis in Sri Lanka: Why Your Health Depends on Understanding This Now
What the Report Actually Shows and What is Pan-Resistant Bacteria
The culture was taken from a blood specimen of a newborn (age recorded as 0). The organism identified is Klebsiella sp., a Gram-negative bacterium notorious for causing severe infections in newborns, particularly in neonatal intensive care units. The incubation time was only 9.6 hours, indicating rapid growth. Every antibiotic on the panel from common first-line drugs to powerful carbapenems was marked “R” for resistant.
In medical terms, this is described as pan-resistant or extensively drug-resistant (XDR) Klebsiella. Such strains are extremely difficult to treat, often requiring experimental or highly toxic combinations that may still fail, especially in fragile newborns whose immune systems are not fully developed.
Why This Matters for Sri Lanka
Sri Lanka has been monitoring AMR for years through the National Antimicrobial Resistance Surveillance Programme. Recent data from the Ministry of Health and major hospitals show worrying trends:
- Carbapenem-resistant Klebsiella pneumoniae (a key member of this group) has increased significantly in both adult and paediatric wards.
- Neonatal bloodstream infections caused by resistant Gram-negative bacteria are rising, contributing to higher morbidity and mortality in intensive care units.
- Resistance rates to last-resort antibiotics such as colistin and carbapenems have climbed in several sentinel hospitals over the past three years.
The appearance of a pan-resistant strain in a newborn’s blood is particularly alarming because neonates have fewer safe treatment options. Many powerful antibiotics are either contraindicated or carry high risks in this age group. When even meropenem and imipenem, the drugs doctors reach for in life-threatening infections – fail, the consequences can be devastating.
The Root Causes: Careless Antibiotic Use and Weak Controls
The main driver behind this crisis is well-documented: overuse and misuse of antibiotics. In Sri Lanka, antibiotics are still widely available without prescription in many pharmacies, despite regulations. Patients often demand them for viral infections such as the common cold or simple diarrhoea, where they have no effect. Doctors sometimes prescribe broad-spectrum drugs “just in case,” and incomplete courses allow surviving bacteria to develop resistance.
Agricultural and livestock use adds to the problem. Antibiotics given to animals for growth promotion or routine prevention eventually enter the food chain and environment, creating additional selection pressure for resistant strains.
Hospital infection control also plays a role. Overcrowded wards, inadequate hand hygiene, and insufficient isolation facilities allow resistant bacteria to spread easily from patient to patient – especially vulnerable newborns.
The Human and Economic Cost
When ordinary infections become untreatable, the consequences are severe:
- Longer hospital stays
- Higher treatment costs (often requiring expensive last-line drugs or experimental therapies)
- Increased risk of death, particularly in children, the elderly, and those with weakened immunity
- Greater pressure on already stretched intensive care units
Sri Lanka’s health system has made impressive progress in many areas, but AMR threatens to reverse hard-won gains in child survival and maternal health. The economic burden is also significant prolonged hospitalisation and advanced drugs place extra strain on both families and the public health budget.
What Must Happen Now
This single laboratory report should serve as a wake-up call rather than a cause for panic. The situation is still manageable if decisive action is taken on several fronts:
- Strict enforcement of prescription-only sales of antibiotics at pharmacies.
- National awareness campaigns educating the public that antibiotics do not work against viruses and must be taken exactly as prescribed.
- Strengthened hospital infection prevention and control with better staffing, training, and surveillance.
- Investment in rapid diagnostic tools so doctors can identify the exact bug and the right drug faster, reducing the need for broad-spectrum antibiotics.
- Continued surveillance and research to track resistance patterns and guide treatment guidelines.
Sri Lanka already has a National Action Plan on AMR. The challenge is to move from planning to consistent, visible implementation across pharmacies, hospitals, clinics, and communities.
The infant whose blood culture showed this alarming resistance is a real patient, not a statistic. Behind every such report is a family desperate for their child to recover. Stories like this remind us that AMR is not a distant future threat. It is already here, in our hospitals, affecting the most vulnerable among us.
The solution lies not in fear, but in responsibility. Doctors must prescribe wisely. Pharmacists must stop selling antibiotics without prescription. Patients must understand that not every fever or cough needs an antibiotic. And policymakers must ensure that surveillance, infection control, and public education receive the sustained attention and funding they deserve.
The rise of pan-resistant bacteria is a global problem, but it is also a deeply local one for Sri Lanka. How we respond today in our pharmacies, our hospitals, and our homes will determine whether future generations can still rely on medicines that once saved millions of lives.
The time for action is now. Every unnecessary course of antibiotics avoided, every proper hand-washing moment observed, and every policy properly enforced helps protect the antibiotics we still have left. The life of the next newborn may depend on it.
Also in Explained | How Can Sri Lanka Improve Its Mental Health Services Amidst Rising Pressures?
(Image Copyright: Karin Schermbrucker)